Scott E. Morrison
Lameness in Foals
The newborn foal can be affected by many congenital and acquired conditions that influence normal limb function and ambulation. Of all congenital deformities in the foal, congenital musculoskeletal abnormalities are the most common, with flexural and angular deformities being the most frequent congenital causes of lameness. However, not all congenital musculoskeletal deformities will cause lameness in the foal, and some may not become clinically evident until the foal matures and begins training. Acquired conditions in the newborn foal are a response to an event that occurs shortly after birth.
Contractures
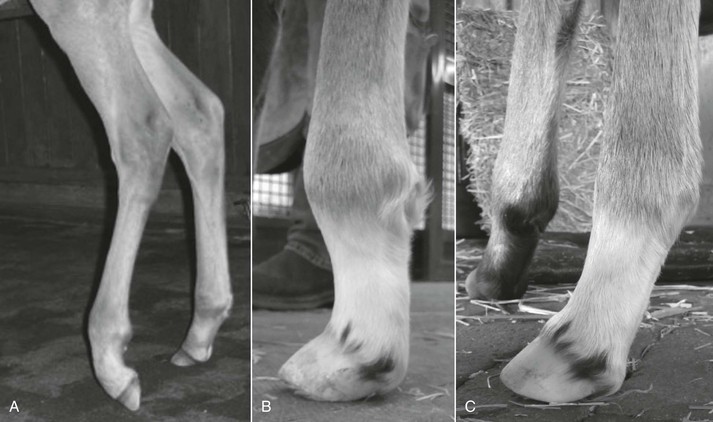
Contractures are congenital conditions that typically affect bigger foals, but they can be seen in all body types. They range from upright fetlocks and pasterns to being over at the knee to severe deformities resulting in loss of use of the limb. One or more limbs can be affected, and the contracture can involve the deep digital or superficial flexor tendon, the suspensory ligament, the joint capsules, or any combination thereof. In foals with deep digital flexor tendon contracture, also known as ballerina syndrome, the heel does not contact the ground, and the foal walks on the toe or dorsal hoof wall. In severe bilateral cases, the foal is unable to stand. With superficial flexor tendon contracture, in contrast, the foot can be placed flat on the ground, but the fetlock and pastern buckle forward (Figure 183-1).
Etiology
The cause of tendon contracture is unknown. Spatial restriction on the growth of large foals in utero is a theory commonly proposed to explain development of contractures, and in support of this was the finding in one study that the placentas of eight Thoroughbred foals with limb contractures were smaller than those of normal foals. There seems to be no correlation between the incidence of contractures and mare age, and the condition does not seem to be inherited. Because flexural deformities seem to be more common in some years than others and appear to come in groups, toxins (locoweed, Sudan grass, iodide toxicosis, or goiter) and influenza infection have been implicated, possibly by causing neuromuscular disorders in the developing limb. Bilateral limb contractures may be part of a larger complex known as contracted foal syndrome, which encompasses multiple developmental disorders, including bilateral limb contracture, torticollis, scoliosis, asymmetry of the skull, and attenuation or thinning of the ventral abdominal wall with possible eventration.
Treatment
Treatment of appendicular contractures consists of medical treatment with oxytetracycline (3 g diluted in 150 mL saline solution and given intravenously over 10 minutes, once daily for 3 days) combined with mechanical stretching of the contracture with splints, braces, or both. Some degree of pain and discomfort can be expected from the splinting process, and administration of antiinflammatory drugs and antiulcer medication should be considered. Contractures become progressively harder to treat successfully with age. For this reason, treating affected foals early and aggressively is imperative; ideally, these foals are evaluated and treated on the first day of life.
The typical newborn foal is sedated with intravenously administered butorphanol (3 mg) combined with xylazine (30 mg) and placed in lateral recumbency in the stall with the eyes covered by a towel. The limb is bandaged with a cotton combine bandage or quilt to the full extent of the contracture. For distal interphalangeal and fetlock contractures, the bandage is applied from the hoof to the proximal part of the cannon bone. For carpal contractures, the limb is bandaged from the cannon bone to the elbow. If the contractures extend from the distal interphalangeal joint through the fetlock and carpus, the bandage must also extend from hoof to elbow. The cotton combine bandage must be firmly secured with Vetrap1 or a similar product. The limb is held in extension, and a 3- or 4-inch-wide roll of fiberglass casting material is unrolled, folded to the length of the bandage, and applied to the palmar or plantar aspect of the limb. While the contracted joints are held in extension by direct manual pressure on the dorsum of the involved joints, the cast splint is bandaged to the limb with adhesive bandaging tape. Care should be taken not to bandage the splint to the limb too tightly or create a wrinkle in the splint material to avoid creating pressure points and skin sores. The pressure and forced extension are held until the cast has set. If the distal interphalangeal joint is involved, the cast splint must be extended to under the solar surface of the foot and at least one third of the way up the dorsal wall of the hoof (Figure 183-2). When the carpus is contracted, care should be taken not to bandage the splint too tightly in the antebrachial region because this can cause radial nerve paralysis.

The splint is usually changed daily, making a new splint and achieving more correction each time. Most cases can be corrected within 3 to 4 days. Foals in which more than one limb is involved may need assistance to stand and nurse. After the limb contracture is corrected with splinting, the leg is maintained in a bandage for a few days to gradually decrease the level of support, and the foal is slowly introduced to turnout and exercise. In the author’s experience, a proportion of these foals will appear normal for a couple of months and then slowly develop an acquired club foot in one of the limbs. For this reason, cases of contracture should be closely monitored throughout their growth and development. Many of these foals eventually become sound athletes.
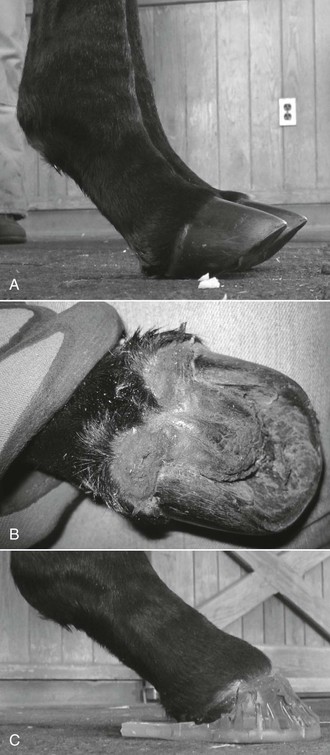
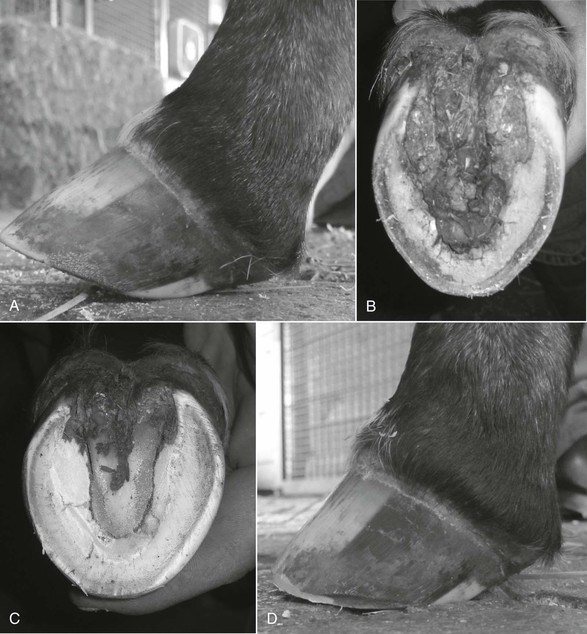
Slight deep digital flexor tendon contracture may respond to stall rest, bandaging, and administration of antiinflammatory drugs. If the toe length is short or is being worn excessively, a toe extension may provide more leverage to lower the heel and stretch the contracted tendon (Figure 183-3). These toe extensions should, however, be used with caution because when they are applied, only a small area of the hoof is being used to counter and correct the contracture. Excessive strain concentrated on the immature toe region can cause tearing of the pedal bone away from the hoof wall, laminitis, or both. Because some cases can develop separation of the anterior part of the coronary band or shear lesion (Figure 183-4), shoes or toe extensions should not be applied within the first week of life, when the soft immature hoof and lamellar interface are more prone to failure. It is much safer to address these cases with bandages and splints, because these methods distribute the stress over a larger area. When toe extensions are used in mild cases, the foal should be monitored daily for lameness, which may indicate lamellar tearing. In those instances, the extension must be removed. In lame foals that have pain in the toe region, radiographs should be taken to rule out mechanical laminitis.


Flexor Tendon Laxity
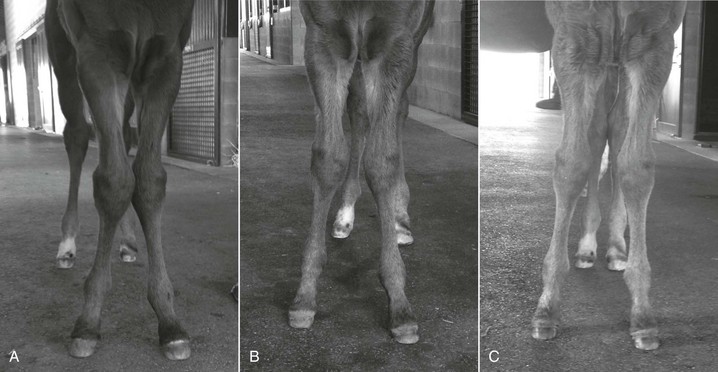
Laxity of the flexor tendons is another congenital condition that typically is seen in dysmature or premature foals, but the condition also occurs in otherwise normal foals. Flexor tendon laxity can affect one or more limbs but usually occurs in the hind limbs (Figure 183-5). The laxity and associated hyperextension commonly involve the phalangeal and metacarpal or metatarsal joints. Some cases also have hyperextension of the carpus or hyperflexion of the tarsus; such animals are said to be “back at the knee” or “sickle hocked,” respectively. Most of these foals improve within the first week of life. Many are also born with excessive hoof growth, so trimming the feet removes toe length, moves the heel position caudally, helps decrease the hyperextension of the distal interphalangeal joint, and helps prevent the toe from turning upward (Figure 183-6). Foals with flexor tendon laxity should be managed with stall rest and controlled exercise, such as hand walking the mare in the barn aisle several times daily while the foal follows. After the muscles and tendons strengthen, the mare and foal can begin turnout into a small paddock. Foals that are back at the knee or sickle hocked should not be allowed to exercise before radiographs have been taken to ensure that the carpal and tarsal bones are fully ossified; crushing of the incompletely ossified carpal or tarsal bones can create permanent wedge-shaped cuboidal bones and lameness. In foals that do not improve within a week or that develop heel bulb ulcerations, heel extensions can help provide caudal leverage and force the toe onto the ground. Heel extensions are usually cuffed shoes, which are attached to the hoof wall with epoxy or acrylic adhesive. These shoes are typically left on for 10 to 14 days, after which the hoof is trimmed and the foal is reevaluated. It is important not to attach the cuff to the heel region of the foot because the area is under stress and easily pinched or bruised by the glue. For this reason, the cuffed shoe should be modified by cutting the cuff away from the back half of the hoof and leaving cuff only to be attached to the toe of the hoof. After the cuff has been on for 5 days, the heel extension can be shortened by 50% with hoof nippers. After another 5 to 9 days, the shoe will need to be removed and the hoof trimmed. Most foals will have strengthened by this time and can be left barefoot. Some may require a second shoe application. If possible, the limbs of foals with tendon laxity should not be bandaged because the additional support causes further relaxation of the tendons and ligaments, worsening the laxity. If a bandage is required to protect an ulcerated area or sore on the fetlock or heel bulb, it should be loosely applied to just that area and not extended up the limb. The occasional foal with severe laxity is unresponsive to treatment (Figure 183-7).

Angular Deformities
Angular deformities can be congenital or acquired and are common in the newborn foal. They are classified as valgus or varus according to whether the limb deviation is lateral or medial to the axis of limb, respectively. Foals with mild deformities are often sound, but those with more severe angular deformities can be lame because the limb instability and abnormal loading of joints causes joint instability, physitis, and abnormal or excessive hoof wear. The normal newborn foal should have a moderate degree of carpal, tarsal, and fetlock joint valgus conformation and slight outward rotation of all four limbs (Figure 183-8). As long as the loading forces on the physis are within the normal physiologic range of the physeal cartilage, most valgus deformities improve with time. This is because physeal cartilage growth increases in response to compressive forces. However, if angular deformities are more severe and compressive forces are excessive, physeal growth slows. Foals with excessive compressive forces usually develop signs of pain and swelling over the medial or lateral region of the growth plate, which is sometimes referred to as physitis.
Angular deformities can be classified as articular, diaphyseal, or physeal in origin. If the deformity can be straightened manually, it is the result of an articular deformity, which can be the consequence of incomplete ossification (usually the carpus or hock), uterine malpositioning, or flaccidity of the periarticular structures. Articular deformities respond well to rest, time, and application of some external form of support such as bandaging and splinting, if the angulation is severe. If incomplete ossification goes unnoticed, it can result in permanent deformity by the time the foal is several weeks old. Diaphyseal angular deformities are less common and originate along the diaphysis of the bone, giving the bone a bowed appearance. Physeal angular deformities are the result of congenital or acquired asymmetric growth of the metaphysis or epiphysis.
Treatment
Treatment of angular deformities depends on severity, location, and how the joint angles change over time. The two main areas of interest with regard to managing the foot are the physis of the distal metacarpus or metatarsus and the physis of the distal radius. The management and treatment goals are to prevent and correct the excessive angular deformities or those that will create excessive compression on the growth plate and retard normal corrective physeal growth. Any varus deformity, and an excessive degree of valgus deformity, is abnormal. Constant improvement or self-correction is the desired trend in response to treatment. Frequent monitoring of the foal is paramount for early detection of limbs that are not improving with time so that proper intervention can be implemented to help correct the deformity. An understanding of the tools available and limitations of each is necessary to effectively implement a foal foot management plan. Equally as important as foot care is recognizing which limb abnormalities will respond favorably to foot manipulations and which may necessitate other treatment modalities, such as transphyseal bridge surgery.
Distal metacarpal or metatarsal angular deformities (fetlock varus or fetlock valgus) are common. Because foot manipulations have most influence on the distal part of the limb and less influence proximally, fetlock angular deformities are most likely to respond to foot trimming or shoeing. Distal physes in the metacarpal and metatarsal bones close by 4 to 5 months and lose 50% of their growth potential every 30 days up to that time. Consequently, it is imperative that fetlock angular limb deformity be appropriately managed at an early age. The goal is to maintain the center of the foot directly perpendicular to the upright cannon bone (imagine a plumb line dropped through the center of the cannon bone to the center of the foot) while ignoring the angulation of the carpus or tarsus. One of the most common mistakes made in treatment of angular deformities is trying to correct a carpal angular deformity by use of foot manipulations at an early age and in the process worsening or creating a fetlock angular deformity. For this reason, emphasis should be on establishing fetlock alignment during the first 3 to 4 months and then, after the distal metacarpal or metatarsal physis has closed, shifting the focus to the carpus because the distal radial physis does not close physiologically until 14 months of age. Valgus deformities of the fetlock usually improve with time and typically do not require treatment unless severe. Fetlock varus, on the other hand, generally does not improve with time and requires trimming, application of shoe extensions, or surgical correction.
Trimming alone can be effective in treating mild angular deformities of the fetlock region. If, however, the self-correcting mechanism is failing to improve the angular deformity, then one must assume that the medial region of the physis in a varus deformity or the lateral aspect of the physis in a valgus deformity is overloaded and growth is decreased in that region of the physis. Trimming and shoeing techniques to help decrease compressive forces on the medial or lateral region of the physis can alter physeal growth and encourage straightening of the limb. For example, lowering the medial side of the foot will decrease compression on the medial aspect of the bone column and increase compression laterally. Decreasing the height of the hoof wall on one side of the limb increases compressive force on the contralateral, longer side and creates tension on the “short” side of the foot, bone column, and physis. Additionally, lowering one side of the foot changes the manner in which the foot strikes the ground and becomes loaded: the longer side of the hoof strikes the ground first, causing the limb to align closer to the long side of the hoof. This potentially encourages loading on the longer side. If the trim alone aligns the foot with the center of the cannon bone, trimming every 2 to 3 weeks may be sufficient to correct the angular deformity.
Care should be taken when trimming foals’ feet. Overtrimming will cause bruising, wing fractures, and lameness. The foot should be routinely examined by digital palpation, and during the trim, as much sole as possible should be left in place for protection. Rolling the edge of the hoof wall can provide some degree of correction without invading sole mass. If the desired foot position cannot be achieved with the trim alone, application of a hoof extension is required. Shoes are recommended in foals that require more than 1 cm of correction and in those that become footsore from corrective trimming. Shoes provide correction while protecting the sole and do not cause focal tearing in one region of the hoof wall (Figure 183-9). If a fetlock deformity does not improve by 60 days and is severe, surgical placement of a transphyseal bridge may be indicated.

< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


