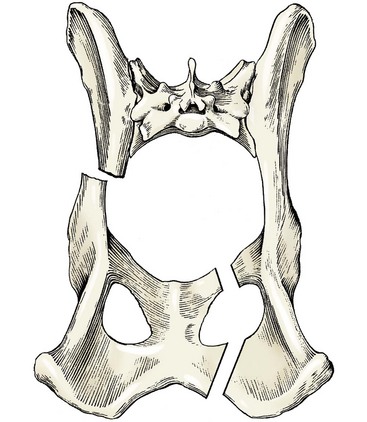
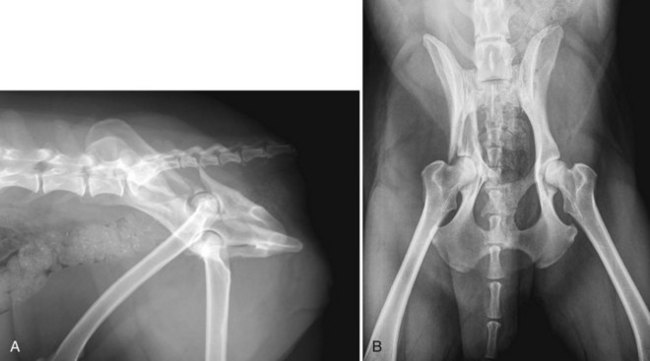
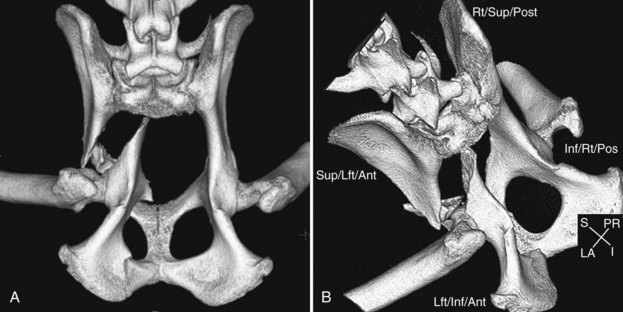
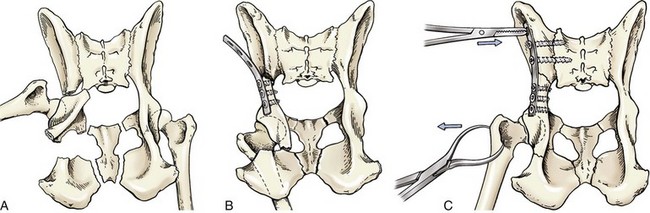
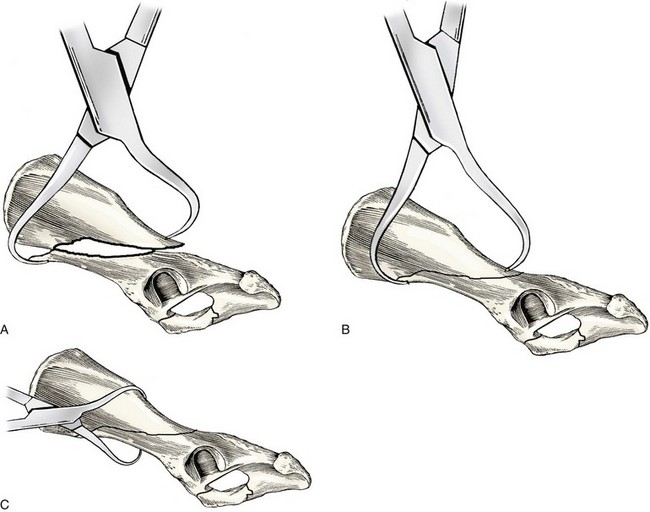
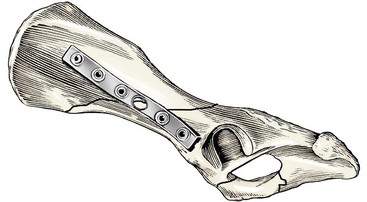
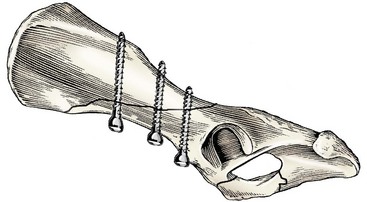
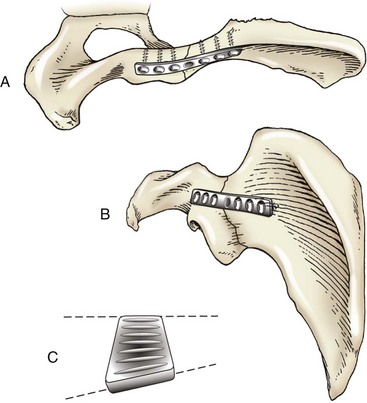
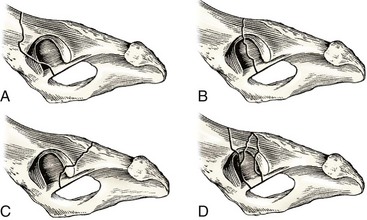
Chapter 57 Fractures of the pelvis are common in companion animals, constituting 16% of all fractures in dogs and 25% of all fractures in cats.28 Of 239 consecutive cases of vehicular trauma in the dog, 20% of all dogs were observed to have pelvic fractures.44 In 100 consecutive cases of trauma of all causes in the cat, 34% were observed to have pelvic fractures.53 Traumatic fracture from automobile-induced injury is the most common cause of pelvic fracture; however, other high energy traumatic incidents, such as falling from a height, account for some pelvic injuries.53 Traumatic injury develops with recognizable clinical patterns, and the distribution of the types and locations of pelvic fractures is no exception. Anatomically, the pelvis may be viewed as a “box-like structure,” with struts through its interior (Figure 57-1). When the pelvis is fractured with displacement, it most commonly fractures in at least three places, with expected patterns observed at the sites of fracture.25 One notable exception is the single nondisplaced stress fracture of the acetabulum observed in racing Greyhounds, caused by the repetitive stress of competitive running.52 Of 556 cats and dogs with traumatic pelvic fractures, 39% had bilateral injuries involving the ilium, acetabulum, or sacroiliac joint.25 Twenty-four percent of the 556 cases had bilateral ilial body fractures, an acetabular fracture with contralateral fracture of the ilial body, or bilateral acetabular fractures. The significance of bilateral injuries is that many patients must undergo multiple and bilateral surgeries with associated surgical morbidity and postoperative concerns to achieve positive clinical results. Injuries to other body systems are commonly associated with vehicular trauma. Of 239 dogs suffering vehicular trauma, 71% had multiple body system injuries with pulmonary trauma (29%), hemoabdomen (15%), soft tissue injury (15%), cardiac arrhythmia (9%), spinal trauma (6%), and urinary tract injury (2%) observed in decreasing order of frequency.44 In another study of 100 dogs with pelvic fractures, 39% had injuries to the urinary tract, with 16% having injury requiring surgery, including ruptured bladder (7%), urethral rupture (5%), and ureteral avulsion (4%).41 In a study of 100 cats presented for vehicular trauma, 53% had thoracic injury, 39% had abdominal injury, and 28% had spinal injury.53 Peripheral nerves in the dog and cat are also at risk in trauma, and those located anatomically close to the pelvis and sacrum may suffer temporary or permanent injury in pelvic fracture trauma. In one report of 34 dogs and cats with peripheral nerve injury, 91% were injuries to the lumbosacral trunk associated with craniomedial displacement of ilial fractures.17 The remainder were associated with acetabular or ischial fractures. Eighty-one percent of animals with peripheral nerve injury had good or excellent neurologic recovery within 16 weeks, and 15% had permanent loss of limb function.17 Injury to nerves that provide voluntary and involuntary control of the urinary bladder and anus may also occur with fractures and luxations of the pelvis, and will be further addressed in sections on sacroiliac fracture-separation and sacral fracture. Serial general physical, orthopedic, and neurologic examinations are important in all polytrauma patients before orthopedic surgical repair. Animals with pelvic fractures should undergo thoracic and additional radiographic studies, depending on the body systems identified as abnormal. Radiographs of the pelvis include standard ventrodorsal and lateral oblique views (Figure 57-2). The purpose of the lateral oblique view is to offset the acetabula and therefore to avoid overlapping images. Computed tomography (CT) is increasingly used to image pelvic fractures (Figure 57-3). Surgical decision making for treatment of pelvic fractures is not found to differ between cases where CT and standard radiographs are used; however, CT is useful to the surgeon in perceiving complex injuries to the acetabulum and sacrum.12 A minimum database may vary for pelvic trauma patients and is dependent upon clinical presentation and time duration since trauma. Complete blood count, serum chemistry profile, urinalysis, and electrocardiogram are commonly performed. Contrast radiography and abdominal ultrasound are used in selected cases. The pelvis is similar to other bones when indications for fracture repair are considered, in that issues of weight bearing, joint alignment, and arthritis secondary to articular fracture are important. Injury to the pelvis includes the additional concern of damage to the rectum and urogenital organs that are housed within the pelvic canal. Malunion and narrowing of the pelvic canal, particularly if the pelvic canal is narrowed by 50% or greater, may result in obstipation or constipation. This is a particular concern for the cat.40 Reconstruction of the pelvic canal for females of breeding age may be important for some patients and clients, but normal parturition can never be assured following pelvic trauma, regardless of surgical fixation. Fractures of the acetabulum, ilium, and luxations of the sacroiliac joint are commonly repaired surgically, whereas fractures of the ischium and pubis are not. Fractures of the acetabulum are repaired to reduce subsequent traumatic arthritis, to restore early weight bearing, and to prevent pelvic canal malunion. Fractures of the ilium and fracture-separations of the sacroiliac joint are repaired to restore early weight bearing and to avoid issues of malalignment of the coxofemoral joint or pelvic malunion. Bilateral pelvic injuries are common, and so bilateral repairs are indicated to distribute early weight bearing to both limbs, rather than overstress an individual fixation. Indications for surgical fixation of ischium and pubis fractures are less common because these bones do not directly support or transmit weight from the femur to the axial skeleton. A pubic fracture may require fixation, as a component of repair of traumatic prepubic tendon rupture. The ischium serves as an important site for muscular origins of the semitendinosus, semimembranosus, and adductor muscles, and avulsion injury of the ischiatic tuberosity may cause persistent lameness.48 Repair is especially recommended in working dogs.48 Fixation methods for ischial fractures are described but are not commonly used, and it is unknown how lack of repair affects long-term function. Cases of pelvic fracture may be carefully selected for nonsurgical or conservative management with reasonable expectations of successful outcome; one report revealed that 75% of dogs attained complete recovery with conservative management.11 Nonsurgical or conservative care consists of cage rest, moderation of activity, appropriate nursing and medical therapy, and physical rehabilitation as the fractures begin to stabilize and function improves. Stable nondisplaced or minimally displaced fractures of the ilium and fracture-separations of the sacroiliac joint may be selected for nonsurgical treatment. Sequential physical and radiographic examinations are indicated in the first 5 to 7 days after trauma because fragment displacement and pelvic canal narrowing may continue to worsen in the days after trauma. If displacement is worsening, a decision to operate can still be made until about 10 days after trauma. Controversy continues as to whether caudal acetabular fractures may be selected for conservative care. This is based on the observation that some dogs with caudal acetabular fracture may present with minimal lameness, compared with acetabular fractures at other locations. One study has shown that secondary arthritis is worse if the fracture is not stabilized, compared with caudal acetabular fractures repaired with a bone plate.6 Financial concerns expressed by clients and chronicity of fractures may force selection of nonsurgical care for cases that otherwise would have clearly benefited from surgery. Malunion, narrowed pelvic canal, and secondary arthritis of the coxofemoral joint may result. Fractures of the ilium are most commonly long oblique fractures of the midbody (Figure 57-4, A). The obliquity is typically oriented from cranioventral to caudodorsal. The location of the fracture can vary and may extend through to the cranial aspect of the ilial wing, or fracture may be located farther caudal with the obliquity over the dorsal aspect of the acetabulum without entering the coxofemoral joint. Comminuted or transverse ilial fractures are also observed, but are much less common than oblique fractures. The caudal fragment of ilium fractures is usually displaced medial and cranial, which compromises pelvic canal diameter and may cause injury to the lumbosacral trunk located just medial to the body of the ilium. Displacement of the caudal fragment in a lateral and cranial direction may also be observed. The surgical approach for common ilial body fractures is a lateral approach, described as the “gluteal roll-up” approach, in which the gluteal muscles are elevated from the lateral and ventral aspect of the ilium and are retracted dorsally.33 This approach allows access to the ilial wing and the body of the ilium, but functionally ends at the cranial aspect of the acetabulum. The surgical approach for repair of caudal ilial fractures that extend dorsal to the acetabulum requires a lateral approach combined with a dorsal surgical approach to the coxofemoral joint.31 Fragment reduction for pelvic fractures, especially in large dogs, requires considerable physical effort from the surgeon and specific strategies that contribute to success. Three strategies may be used for reduction of oblique ilial body fractures; they may be used or combined in any individual case. The first strategy is simple direct fragment manipulation. Bone forceps of appropriate size, depending on animal size, are placed on the caudal fragment. Gentle levering may be used to bring the caudal fragment (displaced medially) to a lateral position, taking care to respect the lumbosacral trunk. The fragments are distracted and reduced, and fixation is applied. This direct approach is most applicable to small dogs and cats. A second strategy is to use the bone plate as an aid in achieving reduction, especially to mobilize the medially displaced caudal fragment out of the pelvic canal (Figure 57-5). Partial reduction can be achieved first with forceps, but it becomes quickly apparent in many large dogs that it is difficult to pull the caudal fragment from its medial position. The plate is properly contoured and then is applied to the caudal fragment with screws. Pressure is directed down on the cranial aspect of the plate with an instrument, and additional screws are placed in sequence, from caudal to cranial, to apply needed force to move the caudal pelvis out of the pelvic canal and achieve reduction. A third reduction strategy uses bone forceps and rotational movement to counteract the overlap of oblique fragments (Figure 57-6). In a procedure described as the forceps sliding maneuver, pointed reduction forceps or speed lock forceps are applied to the overlapping fracture. The forceps are rotated and closed, which forces the oblique fragments to slide into reduction.47 The forceps then hold reduction during plate application. Any individual ilial fracture may require a combination of these three strategies to achieve acceptable reduction. Lateral placement of bone plate fixation is the most commonly used stabilization for ilial body fractures in dogs and cats. External skeletal fixation is described for ilial fixation but is uncommonly used.14 Lateral plating is well accepted for ilial fractures; however, several authors have suggested ventral or dorsal plate positions for improved mechanical stability. A ventral plate position for dogs has been suggested, as the ventral aspect of the ilium is the tension surface during weight bearing.7 The ventral position creates a tension band mechanical environment for the plate and may provide improved stability. A dorsal plate position has been suggested for use in cats, to allow a longer plate to be used with more and longer screws as fixation.16,20 Lateral plating of oblique ilial fractures is optimally accomplished with three screws cranial and caudal to the fracture. At times, only two screws on the caudal side of the fracture are possible because of limited space between the fracture and the acetabulum (Figure 57-7). Cranial ilial wing bone is soft, especially cranial to the sacroiliac joint, and ilial plates tend to loosen cranially. It is important to reduce postoperative cranial plate loosening by having one or two screws penetrate the sacral wing deeply, but stopping short of the spinal canal. It is also important that the lateral plate should have sufficient bending contour throughout its length to match the lateral surface of the ilium. This full contour is essential to pull the caudal fragment from its medially displaced position and to achieve proper reduction of all fracture surfaces (see Figure 57-4, B). Guidelines are available for selection of plate size for dogs and cats of different sizes.30 Typically, 2.7 mm plates are used for cats and small dogs, and 2.7 mm to 3.5 mm plates are used for medium-sized to large dogs. Long oblique ilial body fractures may also be repaired with two to three lag screws (Figure 57-8) placed from ventral to dorsal across the fracture in conjunction with a lateral plate, or as sole fixation.51 Lag screw fixation of the ilium is strong mechanically, but may be difficult to achieve in heavily muscled or obese patients. Plate fixation for caudal oblique ilial fractures that extend dorsal to the acetabulum requires a different plate position and contour method. A straight bone plate may be used for this fixation by locating the plate in a more dorsal position above the acetabulum, compared with the standard lateral position. The plate contour is characterized mostly with a simple twist rather than bending, because of the three-dimensional surface anatomy of the ilium at this location (Figure 57-9). An additional plating method for caudal fractures in dogs and cats is the use of a T-plate.50 The prognosis for fracture healing in plate fixation of ilial fractures is considered to be excellent, and healing allows early return to controlled weight bearing. Loosened screws, especially in cranial plate hole positions in the ilial plate, are commonly seen but have little clinical consequence.7 A ventral plate position in dogs and a dorsal plate position in cats seem to help reduce rates of screw loosening, as do lag screws placed independent of the plate across the obliquity.7,20 Other modes of plate failure, such as bending or breakage of the plate, are rare.7,16 Mild narrowing of the pelvic canal, resulting from inadequate plate contouring or loosened screw fixation, is also common, again with little clinical consequence.7,16 As for all articular fractures, important principles of surgical care of acetabular fractures provide the best results. Perfect reduction of articular fragments and rigid fixation of the fracture are critical for successful treatment. The benefits of appropriate surgical repair include early mobility of the joint and lessening of secondary degenerative arthritis from damaged cartilage. Acetabular fracture types observed are transverse, oblique, and comminuted fractures. Acetabular fractures may be described as fractures through the dorsal rim at cranial, central, and caudal sites (Figure 57-10). Displacement of acetabular fractures is described with reference to the caudal fragment, as this is typically the movable fragment. Displacement is commonly medial with the articular surface rotated dorsally; this opens the fractured joint. The cranial two thirds of the acetabulum has been described to carry most of the weight-bearing forces through the joint, and so fractures at this location are especially important to repair.5,26 It has been observed that upon initial examination after trauma, dogs with caudal one third acetabular fractures may have minimal lameness, and some surgeons decide against surgical fixation. However, long-term follow-up of nonsurgical treatment in cases of caudal acetabular fracture has demonstrated unsatisfactory results from lameness and pain associated with moderate to severe degenerative joint disease.6 Therefore, all locations of acetabular fracture are recommended for surgical repair. The articular cartilage of the acetabulum is C-shaped, with the open part of the C in a ventral location. Repair of acetabular fractures is generally directed at reconstruction of this C-shaped surface, with fixation applied to the dorsal surface above the acetabulum. Transverse, oblique, and comminuted acetabular fractures with a few fragments are generally repairable. Some comminuted fractures have too many pieces, or fragments are too small for effective reconstruction. The surgeon may need to select salvage with femoral head and neck excision, or partial reconstruction of the acetabulum, with the ultimate goal of total hip replacement later after bone healing. Fractures of the medial wall of the acetabulum are often seen in conjunction with fractures of the dorsal rim, and may be associated with subluxation of the femoral head into the pelvic canal. The ligament of the head of the femur is usually intact and attached to a caudal fragment. Reconstruction of the articular surface in the average acetabular repair is usually sufficient to prevent continued medial subluxation of the femoral head, although this is not always the case if the medial wall fracture is severe (Figure 57-11). Acetabular fractures with severe medial wall fracture and continued significant medial displacement of the femoral head are considered unrepairable. Femoral head and neck excision is then advised, or a total hip replacement at a later date may be considered if function is unacceptable.
Fractures of the Pelvis
Fractures of the Ilium
Acetabular Fractures
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


