Chapter 67 Candida species are yeasts that are typically benign counterparts of the normal gastrointestinal, urogenital, and cutaneous flora but can invade tissues and cause disease as a result of disruption of normal host defenses. Candida species can also be isolated from soil, inanimate objects, and hospital environments. The yeasts are small (3 to 6 µm) and ovoid (blastospores) and reproduce by budding. Budding results in the formation of new yeast cells, pseudohyphae (chains of elongated yeast cells), and true septate hyphae. Disease syndromes caused by Candida species that occur in dogs and cats are listed in Box 67-1. More than 200 species of Candida exist, but only a few species have been identified as pathogens in dogs and cats (Table 67-12–10). The most commonly isolated species is Candida albicans, and only C. albicans appears to cause disseminated disease in dogs and cats. Local or disseminated infections where Candida is present with a mixture of bacterial species can occur. Local infections (such as UTIs) with two different Candida species have also been reported.2,11 TABLE 67-1 Candida Species Associated with Disease in Dogs and/or Cats 2–10 When compared with human patients, candidiasis is uncommonly described in dogs and cats. Predisposing factors in dogs or cats with local or disseminated candidiasis have included diabetes mellitus,2,3,12 treatment with immunosuppressive drugs or broad-spectrum antibacterial drugs,2,13 a history of gastrointestinal surgery,4,5 parvoviral infections,14–16 and/or underlying malignancy.2,17 Often more than one of these factors is in the history. Disseminated candidiasis has most often been described in dogs, but also occurs in cats.5,18 Although most animals have underlying immunocompromising conditions, disseminated candidiasis has been described in apparently immunocompetent animals,19,20 which may reflect an unidentified underlying genetic immunodeficiency. Cats with candidiasis usually test negative for FeLV or FIV infection. Analysis of the author’s hospital population suggests that cats are at least as likely as dogs to develop Candida UTIs.11 In other studies, Candida species were isolated from the urine of 0.2% of more than 8000 dogs with UTIs21 and 0.2% of more than 2000 dogs with persistent or recurrent UTIs.22 Urethrostomy or indwelling cystostomy tube placement may be in the history of some cats and dogs with Candida UTIs, respectively.2,6 Local mucocutaneous infections can occur at the site of long-term placement of feeding tubes.7 Disruption of normal barriers is necessary to allow Candida spp. to invade the host. Concurrent use of broad-spectrum antibiotics suppresses the normal bacterial flora and allows Candida to proliferate, which increases the risk that organisms will be introduced into tissues. Candida can adhere to a variety of tissue components such as epithelial and endothelial cells, fibronectin, and thrombi, as well as other bacteria and inanimate objects such as catheters.23 The yeasts can also form biofilms on medical devices and produce a huge variety of hydrolytic enzymes. Within tissues, neutrophils are a key defense against Candida.24 Candida blastospores are phagocytized and destroyed by neutrophils. Mononuclear cells play a less important role. Reactive oxygen species, hydrolytic enzymes, and antimicrobial peptides contribute to the intracellular destruction of blastospores by neutrophils. Thus, any condition that impairs neutrophil numbers or function, such as neutropenia or diabetes mellitus, predisposes dogs and cats to candidiasis. A large number of other cytokines, complement, dendritic cells, and lymphocytes are also involved in the immune response to Candida.24 The formation of hyphae by Candida promotes tissue invasion, which may be followed by life-threatening fungemia and dissemination to multiple organs. This ability of Candida to change its morphology (“morphologic dimorphism”) is thought to be an important virulence factor. Lower urinary tract candidiasis may be subclinical or associated with dysuria, stranguria, and/or hematuria. Systemic signs of pyrexia, lethargy, inappetence, and weight loss have also been described in affected dogs and cats,6 but these signs may result from the presence of other predisposing diseases. Ascending infections may lead to development of Candida pyelonephritis. Overgrowth of Candida in the gastrointestinal tract may occur in animals that are immunosuppressed or treated with glucocorticoids and/or broad-spectrum antibacterial drugs. In some cases, invasion of the mucosa into the lamina propria or deeper tissues occurs (e.g., intestinal candidiasis). Intestinal candidiasis is occasionally identified at necropsy in puppies that die after treatment for parvoviral enteritis and may be a reason for persistent vomiting, diarrhea, and death despite aggressive fluid and antibacterial drug therapy.14 Candida spp. may also contribute to ulcerative glossitis in puppies with parvovirus infection (Figure 67-1). FIGURE 67-1 A, Tongue ulcerations at necropsy in a 2-month-old mixed-breed puppy that was euthanized because of canine parvoviral infection. Candida peritonitis can follow intestinal surgery, treatment with broad-spectrum antibacterial drugs, and subsequent enterotomy site dehiscence.4,5 Mixed infections with Candida and intestinal flora may develop. Affected dogs are febrile, have abdominal pain, and may have other gastrointestinal signs such as vomiting and diarrhea. Disseminated candidiasis results from hematogenous spread of Candida from intestinal, urinary, or possibly corneal or cutaneous sites.12,15,25A diagnosis of disseminated candidiasis should be considered whenever Candida infections are identified in the eye, skin, or urinary tract of an animal that has (or subsequently develops) severe systemic illness. Clinical signs of disseminated candidiasis in dogs include fever, inappetence, anorexia, weight loss, and a variety of other clinical signs that reflect underlying immunosuppressive disease processes and specific organs involved. The latter can include the pancreas, liver, mesentery, spleen, kidneys, heart, lungs, lymph nodes, and, less often, the bone, intestinal tract, eyes, meninges, thyroid, and/or prostate gland.3,12,15,17,20,25–28 Ocular signs in animals with disseminated disease include keratitis and corneal ulceration, uveitis, chorioretinitis, and endophthalmitis.11,12,28 Candida keratitis may also occur as a localized process, sometimes secondary to aggressive treatment of corneal ulceration secondary to other disease processes with topical broad-spectrum antibacterial drugs. Thromboembolic disease may complicate disseminated infections. Pulmonary thromboembolism may result in respiratory distress and death.3,11 Laboratory abnormalities in dogs and cats with candidiasis result from the underlying disease process (such as diabetes mellitus or systemic neoplastic disease) as well as the location and severity of the fungal infection. Laboratory abnormalities in dogs or cats with Candida UTIs may be absent, or there may be evidence of renal failure with azotemia and isosthenuria. Grossly, urine may contain flocculent white debris. Urinalysis may reveal proteinuria, pyuria, and, in some cases, hematuria and/or Candida fungal elements (see Case Example). Dogs and cats with disseminated candidiasis or Candida peritonitis frequently have had nonregenerative anemia and mild to marked neutrophilia with bandemia and toxic neutrophil changes (in contrast to other deep mycoses, where hematologic abnormalities are often mild or absent). Lymphopenia may be present as a result of underlying immunosuppressive illness or drug therapy. Some dogs are thrombocytopenic and have coagulation abnormalities consistent with disseminated intravascular coagulation.3 Findings on the serum biochemistry panel in dogs with disseminated candidiasis are variable and nonspecific but may include metabolic acidosis, moderate to severe hypoalbuminemia, and increased liver enzyme activities.
Candidiasis
Etiology and Epidemiology
Species
Clinical Manifestations
Candida albicans
Dermatitis, UTI, otitis externa, keratitis, disseminated infections
Candida glabrata (formerly Torulopsis glabrata)
UTI, feeding-tube site infections
Candida krusei
UTI, feeding tube site infections
Candida guilliermondii
UTI, dermatitis
Candida parapsilosis
UTI, otitis, dermatitis
Candida tropicalis
UTI
Candida rugosa
UTI
Clinical Features
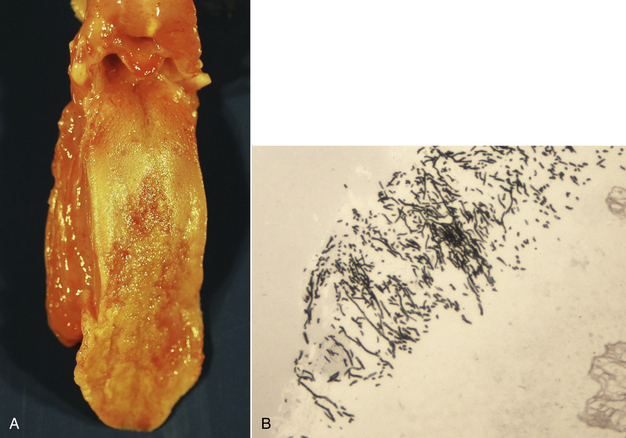
B, Histopathology revealed multifocal ulcerative glossitis, pharyngitis, and esophagitis with intralesional yeasts and pseudohyphae. Gomori’s methenamine silver stain. (Image courtesy University of California Davis Anatomic Pathology Service.)
Diagnosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


