Chapter 8 Auscultation
INTRODUCTION
Despite the lack of gross changes to the tricuspid valve at post mortem examination,1 Stockman, an Edinburgh pathologist, believed tricuspid regurgitation (TR) to be the commonest affliction of the horse.2 This diagnosis made solely by auscultation has been supported by more recent epidemiological studies using Doppler echocardiography.3 However, despite the increased availability of this more sensitive diagnostic technique, auscultation remains the principal means to evaluate the equine heart.4 Opinions differ as to the accuracy of auscultation when used to diagnose cardiac murmurs. Young and Wood3 reported 100% specificity for the diagnosis of mitral regurgitation (MR) and TR whereas Naylor and others5 reported poor accuracy for the diagnosis of a recording of a cardiac murmur; accuracies of 29, 33 and 53% were reported for second year veterinary students, general practitioners and diplomates of a European or American College of internal medicine, respectively. The accuracy of diagnosis was shown to be significantly influenced by training with only diplomates being able to reliably differentiate systolic from diastolic murmurs, although the ability to hear the physical properties of the murmur remained unchanged. However, other authors also believe that a high degree of accuracy can be achieved for the diagnosis of most murmurs in the living animal4,6 and agree that Doppler echocardiography, by increasing our knowledge of the origin of many types of murmur,3,6 has improved teaching and learning, further improving the accuracy of diagnosis by auscultation. This chapter aims to improve diagnostic skill by describing how to differentiate the common cardiac murmurs in horses. Recordings of a variety of cardiac murmurs are presented in the case studies included with this book. However, it must be remembered that the challenge in diagnosis is not in hearing and diagnosing the cause of a cardiac murmur on a recording but in finding and accurately localizing the origin of a murmur in a live animal. With a thorough understanding of normal cardiac physiology, accuracy in diagnosis can be achieved, providing auscultation is undertaken in a quiet environment and sufficient time and thought is put into the examination. A thorough systematic physical examination before reaching for a stethoscope will help in identifying the significance of any cardiac murmurs and prevent such murmurs from being overlooked.
AETIOLOGY OF CARDIAC MURMURS
A murmur is a series of auditory vibrations7 occurring during a normally silent period of the cardiac cycle.8 Murmurs have been attributed to the presence of turbulent blood flow,9,10 periodic wake fluctuations11 or to eddy and vortex formation causing vibration of solid structures.12,13 Murmurs can be associated with congenital cardiac abnormalities,14 and often develop as a result of valvular dysfunction,15 but they are also present in a large number of clinically normal horses.3,16,17,18
Turbulent flow occurs when blood flows at high velocity in wide tubes19 and has been recorded in the aorta of clinically normal horses during ventricular systole and in the left ventricle during rapid filling.20 Murmurs during ventricular ejection and filling are audible in up to 50% and 15% of normal horses, respectively.16 The intensity of these physiological flow murmurs varies and tends to increase with excitement.17 In disease states, e.g. MR and aortic regurgitation (AR) where there is an increase in the blood flow velocities during rapid ventricular filling and ventricular ejection, respectively, flow murmurs may become audible.21 Turbulent flow is also present during increased flow states, e.g. anaemia and exercise.10
Turbulent jets with eddies and vortices at their boundaries are produced when blood flows through narrow orifices into wide channels, as occurs during valvular regurgitation.13 Sound is also thought to be produced by jets directly striking vessel or chamber walls.13
IDENTIFICATION OF NORMAL HEART SOUNDS( EA)
EA)
The first (S1) and second (S2) heart sound can be heard at the level of the apex beat and mark the beginning and end of systole, respectively. The first sound is a relatively long sound compared to S2 and occurs at the onset of ventricular ejection. It is caused by the initial movement of the ventricle, the abrupt arrest of intracardiac blood flow as the atrioventricular (AV) valves tense, and the early part of ejection.16,22 The second heart sound, which is shorter and higher pitched than S1, is caused by the change in direction of blood flow in the aorta and pulmonary trunk at the end of systole, closing the aortic and pulmonary valves.16 In athletic horses with low resting heart rates, two components of S2 (of pulmonic and aortic origin) can often be distinguished when the stethoscope is positioned over the pulmonary valve area. However, two separate sounds can only be heard if they are separated by more than 30 ms,23 which only occurs at low heart rates. There is marked variation between individual clinicians in their ability to distinguish sounds that are close together; however, this does not influence their ability to accurately diagnose the cause of cardiac murmurs. Very marked separation or differences in intensity of the two components of S2 may occur in disease states, e.g. pulmonary hypertension.
The third heart sound (S3) is commonly heard in Thoroughbred-type horses. It occurs at the end of the active relaxation of the ventricle and is associated with the abrupt checking of the outward movement of the ventricular walls.22 It can be differentiated from a split S2 by the different location in which it is heard and its timing. The third heart sound is commonly heard at or slightly caudal and dorsal to the apex beat, whereas a split S2 is heard cranially over the pulmonary valve area. The two components of S2 are temporally very close together and of similar frequency whereas S2 and S3 are more widely separated with S3 being of lower frequency (Fig. 8.1). The intensity of S3 is often increased in horses with atrial fibrillation and in those with very severe MR.24 ( AF, RCT, VMD)
AF, RCT, VMD)
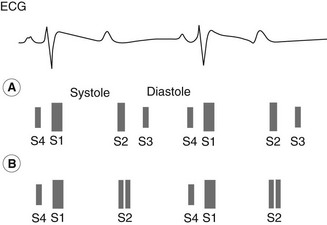
The fourth heart sound (S4) is associated with the transient closure of the AV valves following the atrial contraction and the sudden checking of the distended ventricle.16 It is commonly heard in Thoroughbred-type horses closely preceding S1 (see Fig. 8.1) but is heard less commonly in ponies. An earlier group of vibrations associated with the atrial contractions and AV blood flow is not normally audible at the thoracic wall. A split S1, where the two sounds are of similar frequencies, is less commonly heard and is due to separation of the sounds originating from the left and right ventricle. This is most commonly identified in horses with atrial fibrillation where the atrial contraction and S4 is absent. This can cause difficulties in diagnosis as the split S1 can be mistakenly identified as S4 and S1.
The choice of stethoscope will not limit the cardiac examination as much as the amount of care and thought taken using it; however, various factors should be considered. Higher frequency sounds (e.g. S1 and S2, and AV valve regurgitation) are damped by a large volume of air between the chest and the ear piece.7 Thicker and shorter tubing decreases the audibility of extraneous noise; therefore, short stethoscopes 10–12 inches (25–30 cm) are advantageous.7 The diaphragm of the stethoscope damps out lower frequency sound whereas the bell of the stethoscope is more suitable for detecting these sounds (e.g. S3 and S4, and diastolic murmurs). Cardiovascular sounds and murmurs are usually in the range 20–1000 Hz but the human ear is most sensitive within the range 1000–4000 Hz. Due to the decreased sensitivity of the human ear to low frequency sounds these must be of greater amplitude to reach the threshold of audibility of a sound of higher frequency.25 Sensor-based electronic stethoscopes are now available which allow the operator to increase the amplitude of detected sounds and to select the frequency range over which they wish to listen. A frequency range of 20–420 Hz has been set by one manufacturer to correspond to the “bell” of the stethoscope for the detection of most heart sounds and murmurs, whereas 350–1900 Hz is used to represent the diaphragm mode to detect higher frequency sounds (high frequency murmurs, clicks, ejection sounds and lung sounds). Sensor-based stethoscopes allow data to be stored digitally and replayed or analysed at a later date.
IDENTIFICATION OF MURMURS
The differentiation of the various cardiac murmurs in horses can be difficult: especially the systolic murmurs that are the most common, and can arise from a number of sites.26,27 In addition to the high prevalence of physiological flow murmurs in horses,17,18,26 MR and TR have been shown to develop in Standardbred28 and Thoroughbred racehorses in response to training with up to 30% of normal young Thoroughbred racehorses affected.3 Reduced athletic performance is also common in racehorses but it is important to recognize that cardiac murmurs are often an incidental finding in these horses.29 Recently there has been extensive research on the relationship of cardiac murmurs to performance;30 murmurs of AV regurgitation are not necessarily associated with performance limitations and this is discussed in more detail in Chapter 16.
Location( EA)
EA)
The point of maximum intensity (PMI) of a cardiac murmur is generally located over the site of turbulence,7 and gives an indication of the origin of the murmur.4,8,31,32 As most cardiac murmurs in horses originate from the cardiac valves, it is important to be able to relate the PMI of any murmur to the location of the cardiac valves. The apex beat, which can be palpated over the left thoracic wall at the level of the olecranon process, locates the PMI of sounds originating at the mitral valve (mitral valve area) and a murmur of MR will be heard most clearly at this location.4,8
Once the apex beat is located the other valve areas can be identified from changes in the intensity of the heart sounds. The first heart sound is heard most clearly over the apex beat, whereas S2 is heard most clearly dorsal and cranial to the apex beat. This is the site to which sounds originating at the aortic valve most commonly radiate. Sounds originating from the pulmonary valve are audible cranial and ventral to the aortic valve area with the stethoscope pushed cranial beneath the triceps mass. The pulmonary valve area can be identified more precisely in horses where a split S2 can be heard (see Fig. 8.1).
Timing( EA)
EA)
The causes of cardiac murmurs can be further differentiated from their timing within the cardiac cycle.22,32 Murmurs may be systolic ( AF, IE, RCT, RSD, SFP, VMD, VSD), diastolic (
AF, IE, RCT, RSD, SFP, VMD, VSD), diastolic ( AF, AR, CCD, IE, RSD) or continuous (
AF, AR, CCD, IE, RSD) or continuous ( AF). Once the stethoscope is located over the apex beat it should be moved around until S1 is heard most clearly. The clinician should then listen to the rate and rhythm, identify the heart sounds present and then listen to systole (the period between S1 and S2) and diastole (the period between S2 and S1) for the presence of cardiac murmurs.33 This process should then be repeated as the stethoscope is moved over the other valve areas. The underlying heart rhythm can then be identified and superimposed on the murmur to confirm timing. If it is still difficult to differentiate systole from diastole due to the heart sounds being obscured by a murmur, it is helpful to remember that diastole is longer than systole therefore a very long murmur is more often diastolic (see Fig. 8.1). If the heart sounds are obscured by a murmur such that systole and diastole cannot be identified, it is helpful to find a location where the heart sounds can still be heard and the murmur is less prominent or to palpate the arterial pulses while asculating the heart: a systolic murmur will be coincident with the pulse whereas a diastolic murmur alternates with the pulse. The heart rate and the regularity of the underlying rhythm should always be recorded as this will help in appreciating the significance of any cardiac murmur. A horse in congestive cardiac failure will have an increased heart rate 60–70 beats per minute. Disturbances in cardiac rhythm are discussed more fully in Chapter 13.
AF). Once the stethoscope is located over the apex beat it should be moved around until S1 is heard most clearly. The clinician should then listen to the rate and rhythm, identify the heart sounds present and then listen to systole (the period between S1 and S2) and diastole (the period between S2 and S1) for the presence of cardiac murmurs.33 This process should then be repeated as the stethoscope is moved over the other valve areas. The underlying heart rhythm can then be identified and superimposed on the murmur to confirm timing. If it is still difficult to differentiate systole from diastole due to the heart sounds being obscured by a murmur, it is helpful to remember that diastole is longer than systole therefore a very long murmur is more often diastolic (see Fig. 8.1). If the heart sounds are obscured by a murmur such that systole and diastole cannot be identified, it is helpful to find a location where the heart sounds can still be heard and the murmur is less prominent or to palpate the arterial pulses while asculating the heart: a systolic murmur will be coincident with the pulse whereas a diastolic murmur alternates with the pulse. The heart rate and the regularity of the underlying rhythm should always be recorded as this will help in appreciating the significance of any cardiac murmur. A horse in congestive cardiac failure will have an increased heart rate 60–70 beats per minute. Disturbances in cardiac rhythm are discussed more fully in Chapter 13.
Systolic murmurs result as blood regurgitates through incompetent AV (mitral and tricuspid) valves or as blood is ejected through the semilunar (aortic and pulmonic) valves. MR and TR are common causes of systolic murmurs in adult horses.16–18,26–28,30 Systolic ejection murmurs occur when there is increased flow through the semilunar valves, obstruction to ventricular outflow (valve stenosis), valvular damage without stenosis or dilatation of the vessel beyond the valve.34 Systolic ejection murmurs have been recorded over the aorta and pulmonary artery in clinically normal horses. Aortic and pulmonic stenosis, although common in man7 and dogs,35 have been rarely reported in horses.4 Pulmonic stenosis has been reported in foals with multiple cardiac abnormalities related to tetralogy of Fallot36,37 but hardly ever presents as an isolated finding.38,39
Due to variations in terminology, there is confusion in the veterinary literature as to the incidence of aortic stenosis in horses. Congenital stenosis of the aortic valve is a rare occurrence.16,40–43 However, acquired stenosis may develop in cases of endocarditis4,42 and a relative stenosis can occur due to increased blood flow through the valve, in cases with severe AR.21 Confirmed reports of aortic stenosis causing obstruction to blood flow are rare.44
Diastolic murmurs can be divided into three categories: atrial systolic murmurs (presystolic) occurring between S4 and S1, ventricular filling murmurs occurring between S2 and S3, and regurgitant murmurs from the aortic and pulmonary valves.34 Presystolic murmurs and ventricular filling murmurs are audible in clinically normal horses.16,17,18,26–28 Stenosis of the AV valves is extremely rare; therefore, the most likely cause of a diastolic murmur extending beyond the third heart sound is incompetence or regurgitation of the semilunar valves – most likely the aortic valve.
Continuous murmurs start in systole and extend through S2 into diastole.8 They result from aortopulmonary, aortocardiac or arteriovenous connections or from flow disturbances in arteries and veins. The most common aortopulmonary connection is the patent ductus arteriosus although in adult horses, a murmur audible throughout systole and diastole is more likely to be due to a combination of two or more separate murmurs. ( ACF)
ACF)
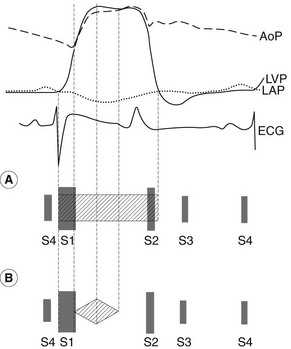
Differentiation of the timing within systole and diastole can further aid diagnosis. Ejection murmurs are early to mid systolic and end before S2,16,34 whereas regurgitant murmurs may occur at any time during systole (early, mid, late) and may extend beyond S2. This can be easily understood by reference to the pressure changes in the heart and great vessels during the cardiac cycle (Fig. 8.2), although there is some confusion in the terminology used to describe these murmurs. The term pansystolic describes a murmur which begins with or replaces S1, continues throughout systole and ends beyond S2, whereas the term holosystolic describes a murmur which starts at the end of S1 and continues to the start of S2, although some authors use the terms interchangeably.25 Murmurs that last throughout systole and extend beyond S2 are likely to be of greater clinical significance than those murmurs which occupy only part of systole45 and it is helpful to reserve the term pansystolic to describe these longer murmurs as this represents clinically important information.
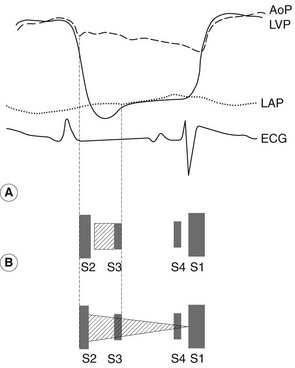
Diastolic murmurs associated with ventricular filling end with S3, which marks the end of rapid filling caused by active relaxation of the ventricle, whereas the murmur of AR is often present throughout diastole15,46 (Fig. 8.3). In order to differentiate these murmurs and the presystolic murmur, it is necessary to be able to identify the normal heart sounds and be aware of the normal timing of these sounds, so that murmurs can be diagnosed in horses in which S3 and S4 are not readily audible.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


