Figure 31.2 The electrohydraulic shockwave fiber (F) is introduced into the biopsy channel of the endoscope and brought in contact with the calculus (A). Spark Generator Riwolith 2280 (Richard Wolf GmbH, Knittlingen, Germany) (B).
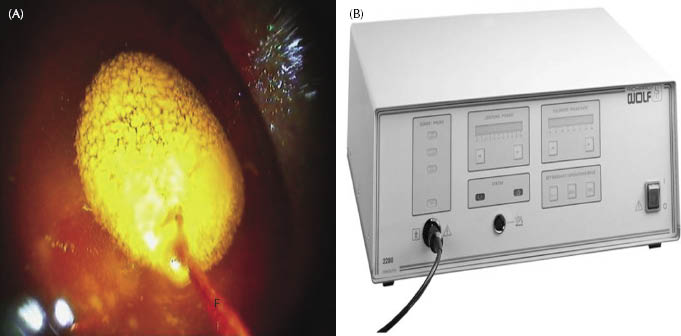
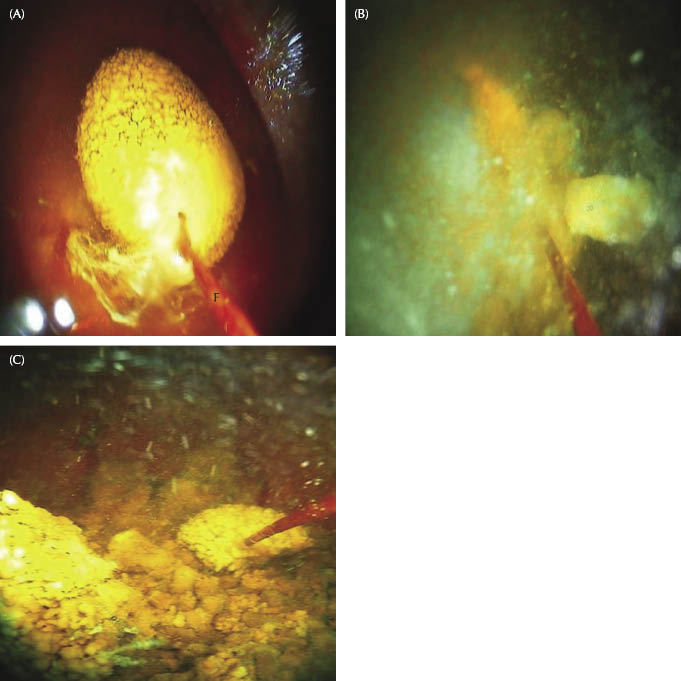
Figure 31.3 Disruption of the calculus into small fragments is achieved by repeated movements of the activated fiber (F) across the calculus (A–C).
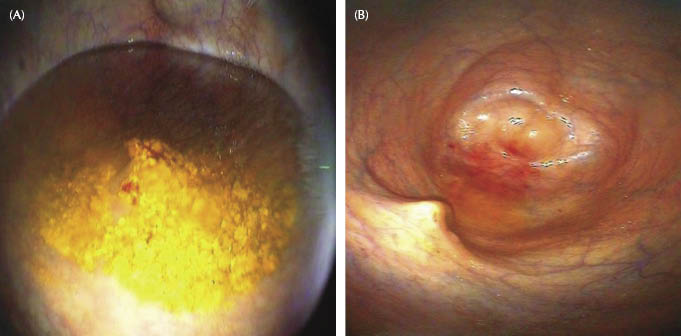
This procedure is continued until none of the fragments are more than 1 cm in diameter. Either the bladder is lavaged with saline solution using an 8-mm-diameter nasogastric tube to facilitate removal of debris, blood clots, and particles at the end of the procedure (Figure 31.4), or the fragments of calculi are left in the bladder where excretion is encouraged by hyperinfusion of Ringer’s lactate (approx. 20 L).
Figure 31.4 Fragmentation is continued until none of the fragments are more than 1 cm in diameter (A). The bladder is then lavaged until all fragments are removed (B).
Laparoscopic-Assisted Cystotomy
The horse is anesthetized and positioned in dorsal recumbency. The penis is exteriorized, cleaned, catheterized with a sterile urinary catheter, and then directed away from the surgical field either caudally between the hind legs or cranially toward the right side.
After aseptic preparation and draping, a 1.5-cm stab incision is made at the umbilicus (Figure 31.5). A 10-mm trocar/cannula system with a safety shield is inserted into the abdomen to facilitate the insertion of a 10-mm-diameter, 50-cm 30° laparoscope. The abdominal cavity is insufflated directly through the cannula system with CO2 to an intra-abdominal pressure of 10–15 mmHg. The surgical table is then tilted to approximately a 30° head-down position to displace the abdominal viscera cranially until the urinary bladder and its associated structures can be visualized (Figure 31.6). After laparoscopic inspection, a 10-mm instrument portal is created under visual control 2–3 cm medial and parallel to the left external inguinal ring. A 10-mm endoscopic grasping forceps is inserted through this portal, and the urinary bladder is grasped at its cranial aspect and elevated to the ventral abdominal body wall (Figure 31.7). Taking the instrument portal as the midpoint, a left parainguinal skin incision is made in a cranial and caudal direction adapted to the anticipated size of the urolith (Figure 31.8). The incision is then continued through all layers of the abdominal wall. The apex of the bladder grasped by the forceps is exteriorized extra-abdominally and held in situ with two stay sutures (1 polyglactin 910) placed on each side of the bladder. The suture bites are about 8–10 cm apart and are fixed through the seromuscular layer. At the same time, the abdomen is desufflated by itself through the mini-laparotomy, and the horse is brought back into a neutral position. A cystotomy is performed between the two stay sutures (Figure 31.9). After urolith removal, the bladder is irrigated extensively with sterile saline (0.9% NaCl) solution to remove all small fragments and blood clots. The incision and the peritoneal cavity are draped for protection, and continuous suction assures that no fluids contaminate the abdominal incision and cavity. With the bladder apex exteriorized, the cystotomy is closed with a two-layer continuous Lembert pattern using 2-0 polyglactin 910 and then rinsed thoroughly with sterile saline (Figure 31.10). After repositioning of the bladder by using a laparoscopic forceps, the umbilical portal site is closed in two layers. The parainguinal mini-laparotomy is then closed in a routine fashion (Figure 31.11).
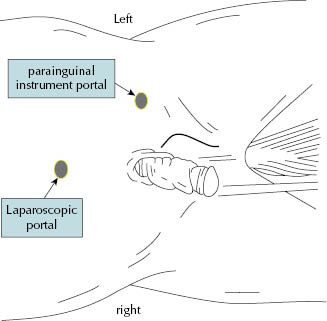
Figure 31.6 Laparoscopic visualization of the urinary bladder and its associated structures after the surgical table is tilted to a 30° head-down position (A,B).
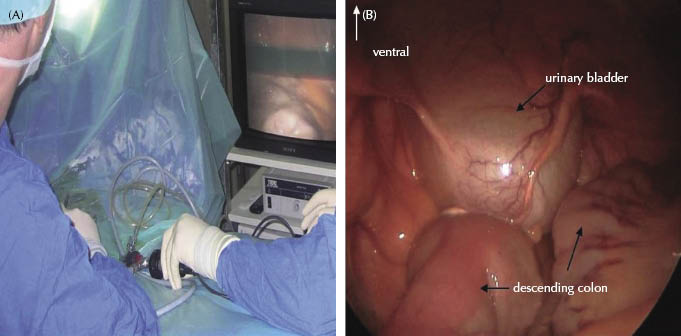
Figure 31.7 An endoscopic grasping forceps is inserted through the parainguinal instrument portal (A). The urinary bladder is grasped at its cranial aspect (B) and elevated to the abdominal body wall (C).
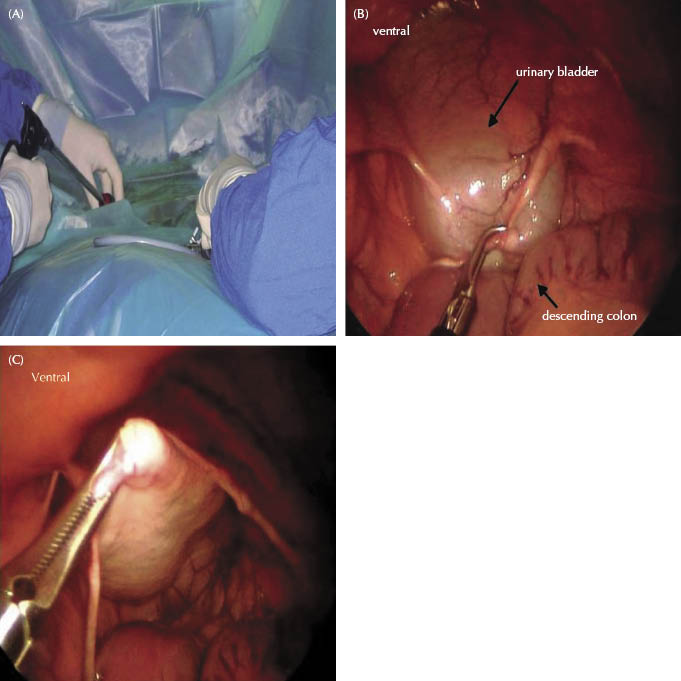
Figure 31.8 Taking the instrument portal as midpoint, a parainguinal skin incision is made, adapted to the anticipated size of the urolith (A–C).
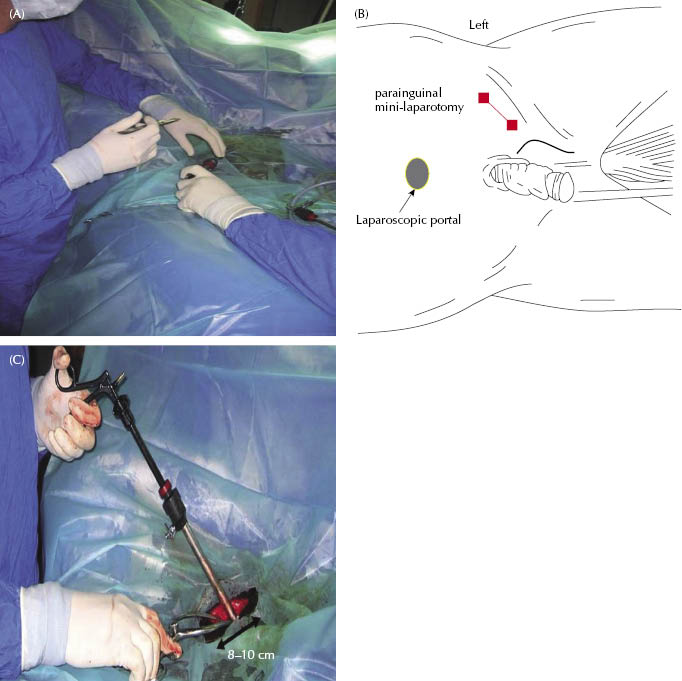
Figure 31.9 The apex of the bladder is exteriorized extra-abdominally and a conventional cystotomy performed for the removal of the urolith (A,B).
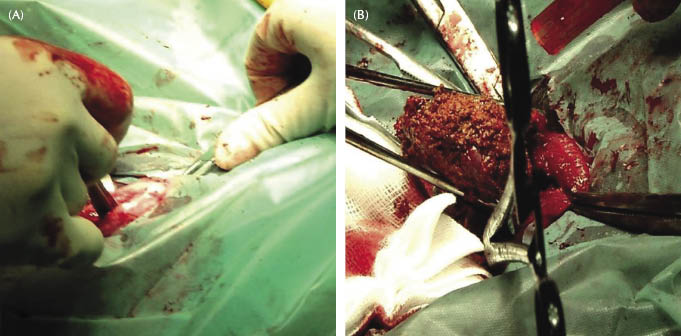
Figure 31.10 (A) Closure of the bladder is performed extracorporeally with a two-layer continuous Lembert pattern. (B) Cystotomy closure is examined for security prior to replacement through the mini-laparatomy.
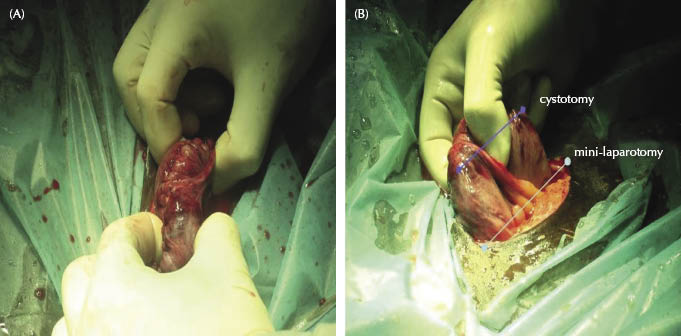
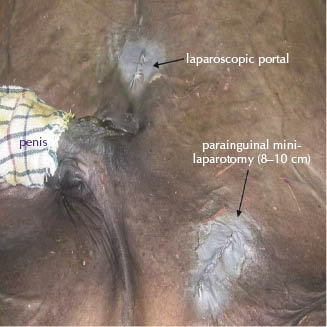
Figure 31.11 Postoperative situation after routine closure of the umbilical portal site and the parainguinal mini-laparotomy.
Laparoscopic Cystotomy (Described by Ragle)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


